You must be signed in to read the rest of this article.
Registration on CDEWorld is free. You may also login to CDEWorld with your DentalAegis.com account.
All teeth are at risk of attack from chemical erosion, and dental erosion is becoming more prevalent among patients treated in dental practices.1 That acid erosion from the ingestion of foods and beverages and within stomach acids produced by the body is a significant problem is suggested by the amount of media advertising for sodas, energy drinks, and fruit juices, as well as medications for heartburn and gastroesophageal reflux disease. It is important that dental professionals who diagnosis dental erosion understand its etiology and be able to provide their patients with insights and guidance on both prevention and treatment. Typically acid erosion of teeth is painless, but for some patients with gingival recession, there is a greater risk of discomfort from dentin hypersensitivity–root sensitivity.
Dental erosion has been defined as the irreversible chemical removal of minerals from the tooth structure.2,3 It is associated with dissolving of the minerals from the tooth enamel and dentin surface, which are effectively softened by acids that are not produced by bacteria. These acids can be from diet, the ingestion of food and beverages, or from stomach acids when they reverse course and travel through the esophagus to the mouth.2-4 These acids can have a significant impact on patients’ oral health by creating loss of tooth structure, tooth sensitivity, changes in the appearance of teeth, and changes in a patient’s bite and occlusion.
Etiology of Dental Erosion
Tooth erosion is very common and has been on the increase during the past 20 years.5 Dental erosion is reportedly present in 34.1% of children and 31.8% of adults, and this trend is increasing significantly.6-8 Dental erosion is not confined to a single etiology; because the loss of tooth substance includes many factors, it is typically due to a combination of conditions. Once the tooth substance is softened, it is more easily worn away when eating, brushing with toothpaste, tooth grinding or bruxing, and in other situations that contribute to loss of tooth structure. Therefore, dental erosion is an important contributor to these pathologies. Dental erosion is caused when acid attacks the teeth. Once the acidity is lower than a pH of 5.5, enamel demineralizes and starts dissolving.9 Sources of acids include those from bacteria that cause caries, acid foods and beverages that are ingested, stomach acids rising through the esophagus into the mouth, and in some cases from outside sources–for example, swallowing water from swimming pools with high concentrations of chlorine,10 breathing in acidic industrial chemicals,11 or tasting wine professionally.12
Acids from food and beverages
While certain beverages and foods are known to be acidic, common eating and drinking habits do not become a problem until the amount ingested increases or the saliva in the mouth no longer provides a diluting or buffering of these acids. Carbonated soda, fruit juices, and sport drinks are very acidic, with pH ranges below 4.0.13-18 Table 1 lists some pH values of beverages.17,19,20 However, it is not a single incidence of drinking these acidic beverages that causes the damage, but their prolonged use.18 Juices with citric acid (eg, orange, grapefruit, and lemon juice) are doubly damaging to tooth enamel because the citrate molecule joins to the calcium ion, reducing the potential of the saliva to remineralize the enamel.21 It has been shown that athletes using sports drinks are not at increased risk of dental erosion compared with the general population: Frequency of use is a more significant contributing factor.20,22
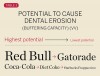
Although much of the focus of dental erosion has been on acidic beverages, dental erosion has also been associated with some common fruits and vegetables with pH levels that fall below the range that contributes to dental erosion (Table 2). Even some routinely used condiments are in the acidic range that can cause tooth damage.19,20 While certain foods and beverages may be more acid than others, there is another factor that contributes to dental erosion—buffering capacity (ie, the amount of the substance needed to reverse the acid pH). The higher the buffering capacity, the greater the potential for dental erosion. Owens evaluated the potential effects of pH and buffering capacity on dental erosion:23 The beverages evaluated for potential to cause dental erosion from the highest to lowest are listed in Table 3. Based upon his results, the lowest pH beverage, Starbucks Frappuccino, had the lowest buffering capacity, (meaning that it had the least potential to cause dental erosion), while Red Bull had the greatest potential to cause dental erosion. In addition to food and beverages, there are a number of acidic medications and supplements—including aspirin and vitamin C supplements—to be considered in relation to dental erosion.24-26
Stomach acid
Stomach acid can reach the oral cavity by regurgitation/reflux and vomiting.27 There is a direct association between gastroesophageal reflux disease (GERD) and dental erosion.27-31 Patients who experience acid reflux as a sour taste in their mouth or heartburn may be taking over-the-counter medications for heartburn to relieve their symptoms. It is important that this information be noted on the patient’s medical history form. Other potential contributors to acid reflux are burping and rumination, which can bring up damaging stomach acid.
Diagnosis
The diagnosis of dental erosion starts with a clinical examination during which changes to the tooth surfaces are recognized, followed by questioning the patient about possible risk factors. Risk factors for dental erosion include:
• frequent ingestion of acidic beverages and foods
• low salivary flow (decreased salivary flow is associated with some medications and aging)
• diagnosis of GERD, regurgitation, vomiting, frequent burping-belching; current or past history of bulimia
• use of chewable acidic medications (aspirin or vitamin C)
• work-related, occupational risks (ingestion or breathing in acidic chemicals)
• use of recreational drugs, such as methylenedioxymethamphetamine (ecstasy) or methamphetamines.
If a patient has risk factors that can contribute to dental erosion, an examination will reveal clinical signs and symptoms of dental erosion. It is unlikely that dental erosion will be seen without other contributing factors. Tooth wear and abrasion typically occur in combination with dental erosion. In the clinical evaluation of tooth surfaces for the diagnosis of erosion, what is typically seen are smooth, shiny surfaces of the teeth where the usual anatomic form of the tooth should be. In patients ingesting very acidic diets, the facial surfaces of anterior teeth are very smooth, and if the beverages being ingested have high sugar content, these teeth may have caries at their facial gingival margins (Figure 1). The occlusal surfaces of posterior teeth in the more advanced stages of erosion due to regurgitation may have extensive exposed dentinal areas with loss of anatomic form (Figure 2). In some cases, the chemical erosion combined with toothbrush–toothpaste abrasion can remove all the enamel, leaving only the dentin exposed (Figure 3). These teeth may exhibit sensitivity. Posterior teeth with restorations may demonstrate fillings that are higher than the surrounding occlusal surfaces of the enamel. Anterior teeth may demonstrate more incisal translucency due to tooth loss at the incisal edge. In patients with the eating disorder bulimia nervosa, who vomit, the hydrochloric acid causes extensive damage to the lingual surfaces of the anterior teeth, where the enamel is lost, leaving exposed dentin (Figure 4).
Prevention and Management
It is essential to educate patients on the consequences of dental erosion. Brochures and handouts about dental erosion, its prevention and treatment, may be placed in the reception area of the dental office. There are many authoritative Internet websites with information that can be used to create individualized in-office handouts. Once the diagnosis of dental erosion has been made, the patient should be offered recommendations for treatment and prevention of further tooth destruction. If dental erosion is allowed to continue, it can lead to loss of function and changes in esthetics. In some cases, it can lead to increased caries risk.
Once the patient is educated to his or her oral condition of dental erosion, its management can be presented. The management of dental erosion should include the following changes or modifications:
1. Change dietary habits to reduce the frequency of ingesting acidic foods and beverages. Use a straw to minimize tooth contact of acidic beverages; rinse the mouth with water after eating or drinking acidic foods and beverages.
2. Discontinue habits of chewing acidic medications or using sucking lozenges for vitamin C.24-26
3. Use of in-office fluoride varnish treatment; use fluoride toothpastes and mouthrinses at home.32
4. Once diseases that contribute to acid erosion are identified, patients should seek medical treatment of GERD, bulimia, gas causing burping, vomiting due to alcohol abuse, etc.33
5. Patients with a sour taste in their mouth should rinse with water or drink milk immediately, or with a liquid antacid to neutralize the stomach acids.32
6. Patients with decreased salivary flow should keep their mouths moisturized with water or oral moisturizers.
7. For sensitivity, use a sensitivity toothpaste with fluoride.
8. To increase tooth resistance to dental erosion, the use of calcium phosphate–containing toothpastes or in-office dispensing of calcium phosphate containing pastes is recommended. 34, 35
9. Use a less abrasive toothpaste and softer bristled toothbrush; brushing should be done before eating or drinking acidic foods and beverages.
10. Patients with identified history of drug abuse should be referred for counseling and treatment.
Conclusion
Dental professionals are seeing more evidence of an increasing rate of dental erosion in their patients. Acidic foods and beverages and the increased presence of GERD are major contributors to this increase in dental erosion. Once a diagnosis has been made, an understanding of the etiology, prevention, and management of dental erosion can help patients maintain their dentition without further damage.
References
1. Ren Y-F. Dental erosion: etiology, diagnosis and prevention. Pennwell Dental Group website. April 2011. http://www.ineedce.com/coursereview.aspx?url=2033%2fPDF%2f1104cei_erosion_web1.pdf&scid=14483. Accessed September 15, 2011.
2. Lussi A, Jaeggi T, Zero D. The role of diet in the aetiology of dental erosion. Caries Res. 2004;38 Suppl 1:34-44.
3. Imfeld T. Dental erosion: definition, classification and links. Eur J Oral Sci. 1996;104 (2[Pt 2]):151-155.
4. Scheutzel P. Etiology of dental erosion—intrinsic factors. Eur J Oral Sci. 1996;104(2[Pt 2]):178-190.
5. Jaeggi T, Lussi A. Prevalence, incidence and distribution of erosion. Monogr Oral Sci. 2006;20:44-65.
6. Dugmore CR. Rock WP. The progression of tooth erosion in a cohort of adolescents of mixed ethnicity. Int J Paediatr Dent. 2003;13(5):295-303.
7. El Aidi H, Bronkhorst EM, Truin GJ. A longitudinal study of tooth erosion in adolescents. J Dent Res. 2008;87(8):731-735.
8. Lussi A, Schaffner M. Progression of and risk factors for dental erosion and wedge-shaped defects over a 6-year period. Caries Res. 2000;34(2):182-187.
9. Hicks J, Garcia-Godoy F, Flaitz C. Biological factors in dental caries enamel structure and the caries process in the dynamic process of demineralization and remineralization (Part 2). J Clin Pediatr Dent. 2004;28(2):119-124.
10. Dawes C, Boroditsky CL. Rapid and severe tooth erosion form swimming in an improperly chlorinated pool: case report. J Can Dent Assoc. 2008;74(4):359-361.
11. Amin WM, Al-Omoush SA, Hattab FN. Oral health status of workers exposed to acid fumes in phosphate and battery industries in Jordan. Int Dent J. 2001;51(3):169-174.
12. Chikte UM, Naidoo S, Kolze TJ, Grobler SR. Patterns of tooth surface loss among winemakers. SADJ. 2005;60(9):370-374.
13. Tahmassebi JF, Duggal MS, Malik-Kotru G, Curzon ME. Soft drinks and dental health: a review of the current literature. J Dent. 2006;34(1):2-11.
14. Owens BM, Kitchens M. The erosive potential of soft drinks on enamel surface substrate: an in vitro scanning microscopy investigation. J Contemp Dent Pract. 2007;8(7):11-20.
15. Ehlen LA, Marshall TA, Qian F, et al. Acidic beverages increase the risk of in vitro tooth erosion. Nutr Res. 2008;28(5):299-303.
16. von Fraunhofer JA, Rogers MM. Effects of sports drinks and other beverages on dental enamel. Gen Dent. 2005;53(1):28-31.
17. Jain P, Nihill P, Sobkowshi J, Agustin MZ. Commercial soft drinks: pH and in vitro dissolution of enamel. Gen Dent. 2007;55(2):150-154.
18. Lussi A, Jäggi T, Schärer S. The influence of different factors on in vitro enamel erosion. Caries Res. 1993;27(5):387-393.
19. Clark DC, Woo G, Silver JG, et al. The influence of frequent ingestion of acids in the diet on treatment for dentin sensitivity. J Can Dent Assoc. 1990;56(12):1101-1103.
20. Lussi A, Jaeggi T. Chemical factors. Monogr Oral Sci. 2006;20:77-87.
21. Meurman JH, ten Cate JM. Pathogenesis and modifying factors of dental erosion. Eur J Oral Sci. 1996;104(2(part 2)):199-206.
22. Mathew T, Casamassimo PS, Hayes JR. Relationship between sports drinks and dental erosion in 304 university athletes in Columbus, Ohio, USA. Caries Res. 2002;36(4):281-287.
23. Owens BM. The potential effects of pH and buffering capacity on dental erosion. Gen Dent. 2007;55(6):527-531.
24. McCracken M, O’Neal SJ. Dental erosion and aspirin headache powders: a clinical report. J Prosthodont. 2000;9(2):95-98.
25. Grace EG, Salani E, Kaplan S. Tooth erosion caused by chewing aspirin. J Am Dent Assoc. 2004;135(7):911-914.
26. Giunta JL. Dental erosion resulting chewable vitamin C tablets. J Am Dent Assoc. 1983; 107(2):253-256.
27. Järvinen V, Meurman JH, Hyvärinen H, et al. Dental erosion and upper gastrointestinal disorders. Oral Surg Oral Med Oral Pathol. 1988;65(3):298-303.
28. Howden GF. Erosion as representing symptoms in hiatus hernia: a case report. Br Dent J. 1971;131(10):455-456.
29. Bartlett DW, Evans DF, Smith BG. Oral regurgitation after reflux provoking meals: a possible cause of dental erosion? J Oral Rehabil. 1997;24(2):102-108.
30. Ali DA, Brown RS, Rodriguez LO, et al. Dental erosion caused by silent gastroesophageal reflux disease. J Am Dent Assoc. 2002;133(6):734-737.
31. Yip KH, Smales RJ, Kaidonis JA. The diagnosis and control of extrinsic acid erosion of tooth substance. Gen Dent. 2003;51(4):350-353.
32. Yip KH, Smales RJ, Kaidonis JA. Management of tooth tissue loss from erosion. Quintessence Int. 2002;33(7):516-520.
33. Lackey MA, Barth J. Gastroesophageal reflux disease: a dental concern. Gen Dent. 2003;51(3):250-254.
34. Muñoz CA, Feller R, Haglund R, et al. Strengthening of tooth enamel by a remineralizating toothpaste after exposure to an acidic soft drink. J Clin Dent. 1999;10(1):17-21.
35. Wegehaupt FJ, Attin T. The role of fluoride and casein phophopeptide/amorphous calcium phosphate in the prevention of erosive/abrasive wear in an in vitro model using hydrochloric acid. Caries Res. 2010;44(4):358-363.
About the Author
Howard E. Strassler, DMD Professor Department of Endodontics, Prosthodontics and Operative Dentistry University of Maryland Dental School Baltimore, Maryland